Staged Development Tool Adapted for Hybrid Workshops to Better Support National Public Health Institutes
The COVID-19 pandemic and travel restrictions spurred an evolution for the Staged Development Tool (SDT), which helps national public health institutes develop roadmaps to achieve a higher level of functioning, from in-person only workshops to a hybrid model. Put to the test in three countries, the approach offers new flexibility and will likely encourage more institutes to use the SDT and take ownership of the SDT process.
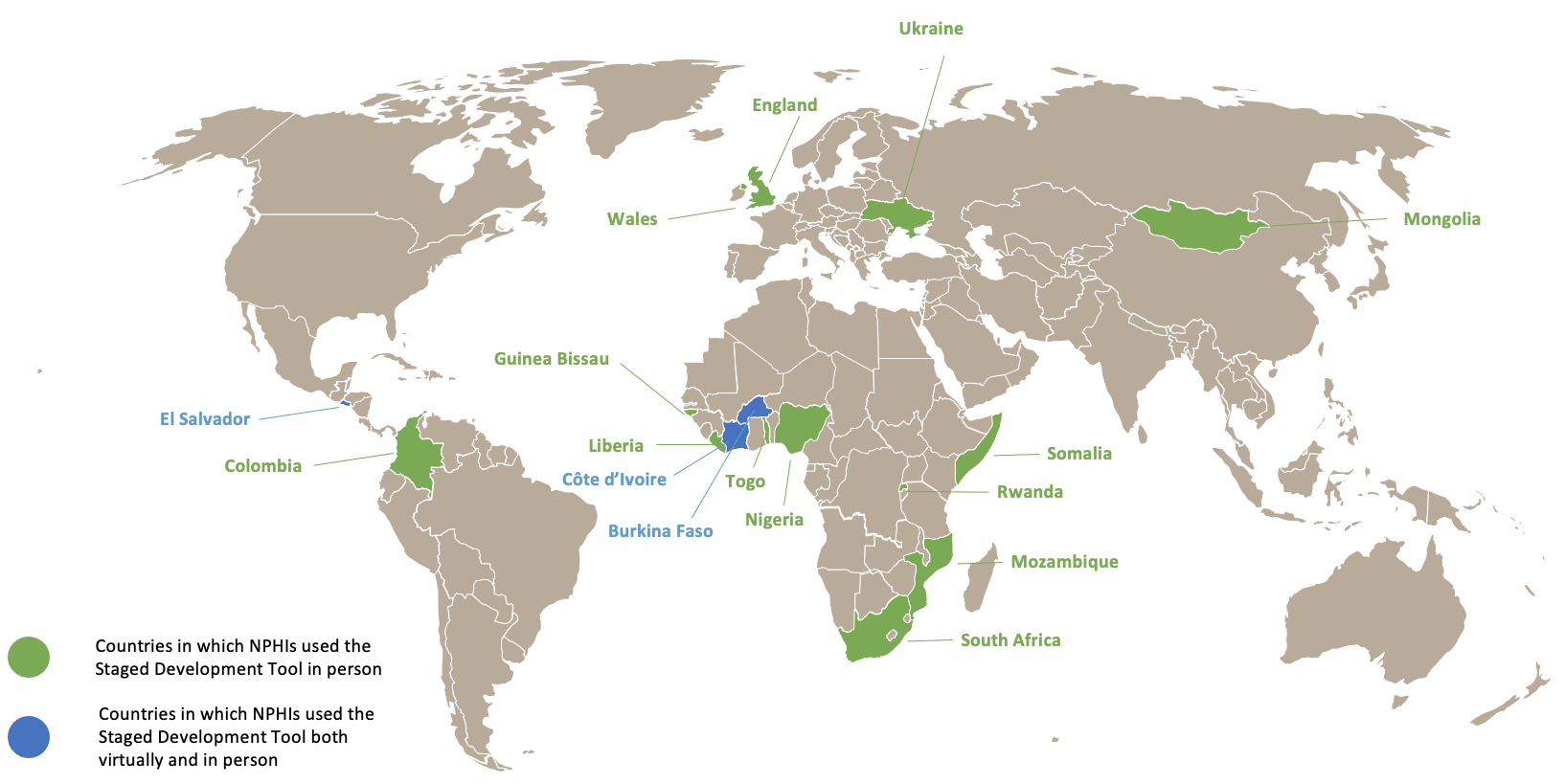
Countries where NPHIs have used the SDT, either in-person or with a mixed approach
The Staged Development Tool was developed in 2017 by IANPHI and the U.S. Centers for Disease Control and Prevention (CDC), in consultation with leaders of national public health institutes (NPHIs) from around the world, and has been used in 18 countries to date. The tool helps NPHIs assess their current capacities, identify and prioritize gaps in functionality, and develop a roadmap for achieving a higher level of functioning.
The SDT is implemented in workshop settings, with participants using detailed discussion guides to clarify their NPHI’s current state, desired state, and major gaps that need to be addressed to move to their ideal state. In the original format, SDT workshops were held in person with facilitators and recorders from IANPHI and U.S. CDC, or trained in person by them. When the COVID-19 outbreak began in early 2020, travel restrictions imposed by many countries made it difficult to hold in-person, facilitated workshops.
In early 2020, when Côte d'Ivoire’s Institut National de Santé Publique (INSP) began planning for an SDT workshop, IANPHI developed a mixed in-person and remote approach for SDT workshops. Because SDT workshops are very interactive, even partially virtual workshops present many technical and logistical challenges. Therefore, the decision was made to simplify the SDT process, especially the way in which the process moves from the assessment stage to prioritization and planning. For example, during in-person workshops, a recorder typically shares what is being discussed on an assessment form. However, doing so in a partially or totally virtual meeting would have precluded participants from seeing each other and reduced interaction. Rather than spending time reviewing the assessment form as a group, the revised process has facilitators and recorders work apart from participants to restructure input from the assessment form to fit a planning form – providing the basis for the prioritization and planning steps of the SDT process. Because of limitations on what can be shared on a computer screen, the forms were also simplified.
Another issue was the need for facilitators and recorders to be trained virtually, since travel for in-person training was not possible. New training materials, as well as step-by-step guides to the simplified process, were developed.
SDT Hybrid Model Put to the Test in Côte d’Ivoire, Burkina Faso and El Salvador
The first SDT hybrid workshop finally took place in September 2020 in Côte d’Ivoire. Côte d’Ivoire’s INSP is a long-standing NPHI and member of IANPHI. The purpose of the SDT workshop was to identify how INSP’s research could achieve a higher level of functioning and to inform a funding proposal to IANPHI and U.S. CDC.
INSP leaders participated in the workshop from Côte d’Ivoire – some gathered together and sharing a microphone, and others elsewhere by themselves – while IANPHI and U.S. CDC facilitators and recorders remained in Atlanta. Several technical issues, for example, the need for participants in the common room to ensure the shared microphone picked up their voices, made facilitation and recording more difficult.
Over many years, the INSP staff had developed common ways of thinking about their work, making it harder to generate the kinds of positive conflict and probing that help uncover underlying causes for barriers to progress. Nevertheless, the INSP team identified several next steps and low-hanging fruit. As a follow-up, INSP’s leadership has since started working on a scope of work with IANPHI and U.S. CDC. The INSP communications team also completed the initial stages of the design and development of a new website, with the technical assistance of the IANPHI communications team.
Burkina Faso’s INSP was formed in 2018, merging several government institutions with strong research capacities. The purpose of the SDT workshop was to bring together leaders of the INSP centers to discuss the data-to-action continuum and ways to enhance the use of INSP’s data to impact public health.
The workshop was conducted in August 2021 over two days, allowing for ideas from the first day to be organized overnight. The second day focused on prioritization, planning and next steps. Because several individuals supporting the workshop were in different time zones, splitting the workshop into two days helped all involved to maintain reasonable working hours. IANPHI staff remotely trained the facilitator, an IANPHI consultant in Burkina Faso, and one recorder from INSP, who were on site. A co-facilitator and additional recorders joined from IANPHI and U.S. CDC in Atlanta. At the end of the workshop, INSP’s leaders agreed on a plan, which included specific needs for technical and funding support and training. INSP has since been working on a scope of work with IANPHI and U.S. CDC to address these needs.
In El Salvador the SDT workshop was implemented by the Council of Ministers of Health of Central American and the Dominican Republic (COMISCA) and the U.S. CDC Central America Office in June and July 2021, to contribute to a formal strategic plan for strengthening the operations of El Salvador’s Instituto Nacional de Salud (INS) and to help INS become a nationally recognized leader in public health.
The onsite facilitator was trained by U.S. CDC, while the recorder was a professional hired by COMISCA specifically for the workshop. U.S. CDC staff also developed a quick reference guide for each of the discussion guides being used, to help the facilitator keep the discussions on track. The main facilitator elected to recruit co-facilitators to assist; the main facilitator would introduce the discussion guides and facilitate through the first two domains, then pass facilitation over to co-facilitators. Given the training and skill needed to lead discussions to concrete next steps, it is recommended that a single facilitator work through a discussion guide rather than multiple facilitators. It is possible to alternate facilitators by having a single facilitator per discussion guide which will minimize repetition of thoughts and makes for more efficient discussions. The proceedings from the SDT workshop were used to inform a strategic plan created by INS to strengthen its capacity to support public health efforts in El Salvador.
Lessons Learned from the SDT Hybrid Model
The first three NPHIs to implement hybrid SDT workshops used creative approaches to ensure success, which may be useful both in future in-person and hybrid workshops. These included quick reference guides developed to help the facilitators stay on track and splitting the workshop into two days – one for assessment and one for planning. The simplified SDT structure and step-by step guide will also be valuable in future workshops, whether in person or hybrid.
Still, there are significant challenges to consider when planning a remote SDT workshop. Carefully planning the information technology (IT) logistics and testing the set up well in advance are pre-requisites to avoid facing significant communication issues, which could hinder the outcomes of the workshop. The IT set up should include a microphone, camera, and keyboard for each participant. This is especially useful when the facilitator is in a different location from the participants. It is difficult to hear when one microphone is shared. The lack of a camera on the person speaking also diminishes the interpersonal connection and it is virtually impossible to “read” gestures and connect the person to the comments.
Hybrid workshops also take longer than anticipated, as the process moves more slowly than it does in-person. Organizers need to plan accordingly and leave more time, both for introductory sessions and for discussions.
Facilitation is also more difficult when the facilitator is not sharing a space with participants. It is particularly the case for facilitators who are new to facilitating and have had less training. They can have a harder time keeping participants on track, getting to the underlying causes and obtaining tangible next steps. Future training should include simulations or other exercises to prepare facilitators to address these issues. Another consideration is the training of the workshop recorder. A recorder who is familiar with the SDT process will produce more concise notes and will be able to quickly highlight the key takeaways from the discussion.
The SDT continues to be useful to foster positive conversations among groups in NPHIs and help them to achieve a shared understanding of their developmental stage and where they would like to be. As a result of the COVID-19 pandemic, there has been greater ownership of the SDT by NPHIs that implement it, leading to a diversity of approaches and experiences. Some of the materials developed for training and to help the facilitators will be valuable as additional NPHIs implement the SDT in person or using a hybrid approach.
NPHIs interested in using the SDT are encouraged to explore information on the IANPHI and CDC websites, and contact us for further information (info@ianphi.org).
Côte d’Ivoire INSP | Burkina Faso INSP | El Salvador INS | |
Discussion Guides used | 28. Public Health Research | 23. Data-to-Action | 1. Planning 2. Leadership and Management 8. Internal Communication |
Dates of workshop(s) | 16 Sept 2020 | 3-4 Aug 2021 | 24 June, 12 July, 15 July, 2021 |
Facilitator locations | Remote | Onsite and remote | Onsite (primary facilitator) and remote |
Recorder locations | Remote | Onsite and remote | Onsite (primary facilitator) and remote |
Participant locations | Some in one room, others remote | In one room | Mostly in one room |
Number of participants | 12 | 13 | 20 |